Shoulder pain is one of those things that’s easy to write off — a bad night’s sleep, too many reps at the gym, or the kind of ache that just comes with getting older. But some shoulder pain is telling you something specific, and ignoring it can turn a manageable injury into a much bigger problem.
Rotator cuff tears are among the most common serious shoulder injuries in adults, and they don’t always announce themselves with dramatic pain. Understanding what rotator cuff tear symptoms actually look and feel like is the first step toward getting the right care before the damage compounds.
What the Rotator Cuff Actually Does
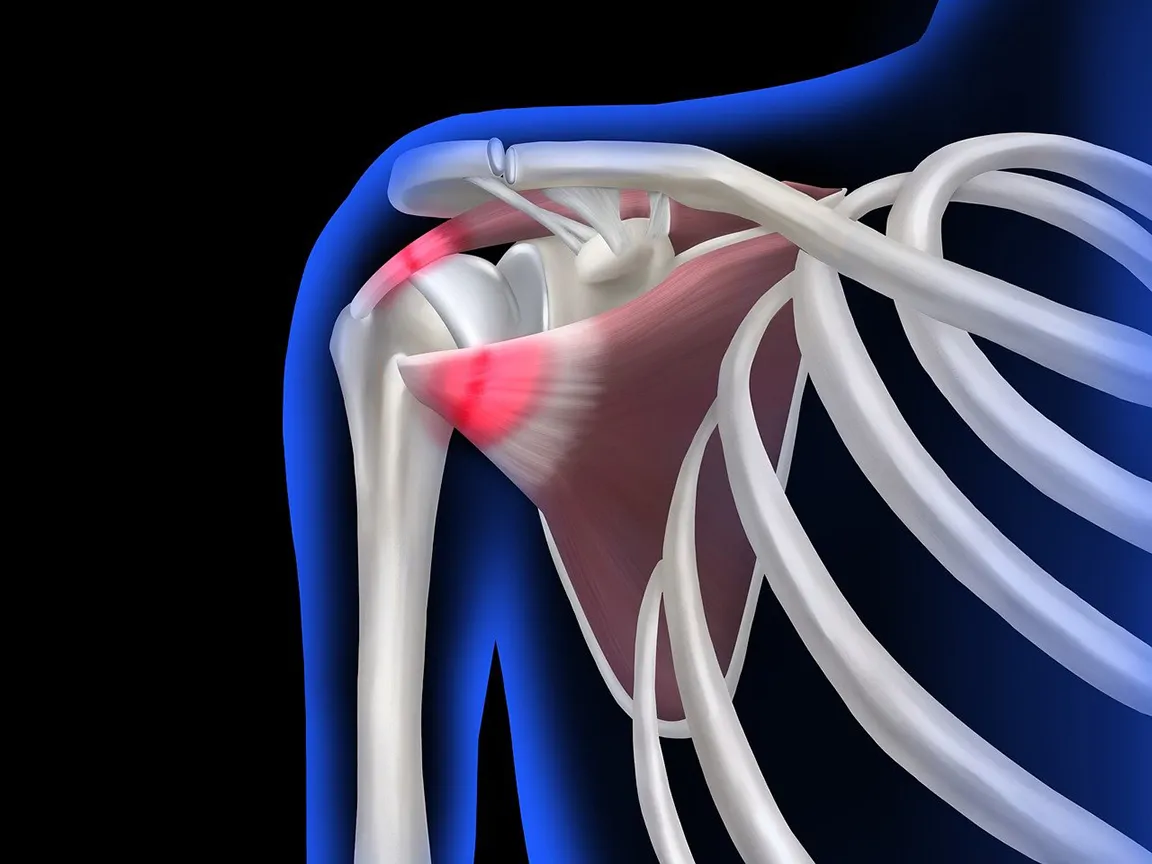
Your rotator cuff is a group of four muscles and their tendons that wrap around the shoulder joint, holding the head of the upper arm bone firmly in the shoulder socket. It’s the reason you can lift a coffee cup, reach a high shelf, or throw a ball — and it’s under constant mechanical stress every time you use your arm.
Because of this, the rotator cuff is uniquely vulnerable. Tears can happen suddenly from a traumatic event, but they also develop slowly over years of repetitive motion, poor posture, or simple age-related wear. By the time symptoms become noticeable, the damage is often already well underway.
The Most Common Rotator Cuff Tear Symptoms
Pain is usually what brings people in — but not all rotator cuff pain feels the same, and its location and behavior can tell you quite a bit.
Most people with a rotator cuff tear describe a deep, aching pain in the shoulder that radiates down the outer arm toward the elbow. It often gets worse with specific movements, particularly reaching overhead, lifting, or rotating the arm outward. Night pain is one of the most telling signs — many people find it difficult or impossible to sleep on the affected side, and some wake up from pain alone.
Beyond aching discomfort, watch for these specific warning signs:
- Weakness when lifting the arm or rotating it away from the body
- A crackling or grinding sensation (called crepitus) with shoulder movement
- Difficulty reaching behind your back, such as when fastening a seatbelt
- A noticeable “drop” in strength compared to your unaffected side
- Loss of active range of motion, even if passive range (someone else moving your arm) remains intact
That last point is clinically significant. If a physical therapist or physician can move your arm through a full range of motion, but you can’t do it yourself, that asymmetry strongly suggests a structural problem with the rotator cuff rather than a joint or capsule issue.
Partial vs. Full-Thickness Tears: Why It Matters
Not every tear is created equal, and the type of tear often determines how symptoms present — and what treatment looks like.
A partial tear means the tendon is damaged but not completely severed. These can produce significant pain and weakness, but many people retain reasonable shoulder function and may initially dismiss the injury as a strain. Full-thickness tears, where the tendon is completely torn through, often cause more dramatic weakness and can make certain movements nearly impossible. Some people with complete tears actually report less constant pain than those with partial tears — the tension on the remaining tissue is gone — but their functional loss is typically more severe.
This distinction matters because the two types follow different recovery trajectories. Partial tears frequently respond well to conservative treatment, while full-thickness tears — especially in younger, active patients — often require surgical evaluation.
Acute vs. Chronic: How the Injury Happened Changes Everything
A weekend athlete who tears their rotator cuff diving for a volleyball is in a very different clinical situation than a 58-year-old who gradually developed shoulder pain over two years of overhead work. Both are dealing with rotator cuff tear symptoms, but the underlying injury, treatment timeline, and prognosis can differ considerably.
Acute tears typically come with sudden, sharp pain at the moment of injury, followed by immediate weakness and difficulty moving the arm. Patients often describe hearing or feeling a pop. Chronic degenerative tears, by contrast, tend to creep in — a dull ache that gradually worsens, stiffness that builds over months, and weakness that seems to appear out of nowhere until one day you realize you can’t lift a gallon of milk without wincing.
Both deserve medical attention. The chronic presentation, ironically, is the one more likely to be delayed — because the gradual onset makes it easier to rationalize away.
When to Stop Waiting It Out
Most people apply heat, rest, and hope before they seek care. That’s understandable. But there are specific scenarios where waiting becomes genuinely risky.
Seek evaluation promptly if your shoulder pain followed a fall, collision, or sudden forceful movement. Acute traumatic tears can be associated with other injuries — labral damage, bicep tendon involvement, or even fractures — that need to be ruled out quickly. Significant, sudden weakness in the arm after an injury is also a red flag that warrants same-week imaging rather than a “let’s see how it feels” approach.
For chronic symptoms, the general rule is this: if shoulder pain has persisted beyond four to six weeks without improvement, or if it’s disrupting your sleep or daily function, it’s time for a professional evaluation. MRI remains the gold standard for diagnosing rotator cuff tears and determining their size and location — information that’s essential for making good treatment decisions.
What Treatment Actually Looks Like
The good news is that rotator cuff tears don’t automatically mean surgery. Many patients — particularly those with partial tears or lower functional demands — respond well to a structured conservative care plan.
Physical therapy focused on rotator cuff strengthening and scapular stabilization can meaningfully reduce pain and restore function. Corticosteroid injections can calm inflammation enough to make therapy more productive. And in some cases, newer regenerative options like platelet-rich plasma (PRP) injections are being explored for their potential to support tendon healing.
Surgical repair is typically reserved for complete tears in active individuals, failed conservative treatment, or cases where the functional loss is significant enough to affect quality of life. Arthroscopic techniques have improved outcomes considerably, with shorter recovery timelines than older open procedures.
The critical variable is timing. Early diagnosis allows more options. Untreated tears can enlarge, and chronically retracted tendons become progressively harder to repair — which is why putting off an evaluation almost never improves the outcome.
Getting the Right Diagnosis in Oklahoma
If any of these rotator cuff tear symptoms sound familiar, the physicians at Access Pain Solutions can help you get clarity. Our team specializes in musculoskeletal pain evaluation and offers a range of treatment options — from conservative management and targeted injections to coordinated surgical referrals when appropriate.
Don’t let shoulder pain limit what you can do. Contact Access Pain Solutions to schedule an evaluation and find out exactly what you’re dealing with.